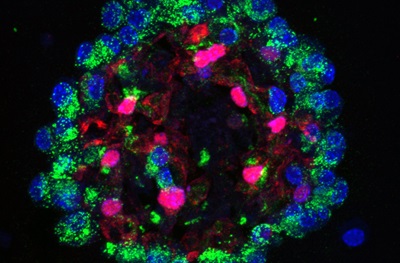
Example of AT2 and AT1 epithelial cell generation in a lung alveolar organoid used to examine MANC and AMP function. Green staining for surfactant protein C indicates AT2 cells whereas red staining for Hopx indicates AT1 cells.
Credit: The lab of Ed Morrisey, PhD, Perelman School of Medicine, University of Pennsylvania
PHILADELPHIA – Details of lung cell molecular pathways that promote or inhibit tissue regeneration were reported by researchers from the
Perelman School of Medicine at the University of Pennsylvania in Cell this week. Their aim is to find new ways to treat lung disorders.
“We need better targets,” said senior author Edward E. Morrisey, PhD, a professor of Cell and Developmental Biology, and director of the Penn Center for Pulmonary Biology. “All we have now are blunt sledge hammers that don’t work” for conditions such as idiopathic pulmonary fibrosis (IPF), a lung disorder whose cause is poorly understood. Knowing the specific cells and pathways that promote repair and regeneration versus scar formation in the lung will help inform the development of more precise and effective therapies.
In 2012, the annual incidence of idiopathic pulmonary fibrosis in the United States was 16 to 17 per 100,000 people. In the United States alone, that translates into 130,000 to 200,000 people affected by IPF. The lung tissue of a person with pulmonary fibrosis becomes damaged and scarred, with thick, stiff tissue making it difficult for the lungs to expand. As it worsens, the patient often has extreme shortness of breath, and the lung, once damaged, is unable to repair itself.
Chronic obstructive pulmonary disease (COPD) is more common than IPF and is characterized by the loss of gas exchange structures in the lungs called alveoli. In the United States, more than 30 million people are affected by COPD and it is quickly becoming a leading cause of disability and death in the world. The ability to balance regeneration of structures such as alveoli with scar formation is essential for proper maintenance of respiratory function.
“The lung is one of the most complex organs in the human body,” Morrisey said, with dozens of cell types, each with specialized roles such as delivering oxygen and eliminating carbon dioxide from blood in the circulatory system (gas exchange). Other cells produce surfactant and mucous to lubricate air spaces for smooth expansion and contraction, and still others create a barrier to pathogens and harmful pollution.
“The complicated structure of lungs is why it is difficult to quickly diagnose the exact type of lung disease a person may have with any certainty,” he said. “Also, as there is considerable reserve capacity in our lungs most people are not diagnosed with lung diseases such as IPF until the disease has progressed significantly.” This biological compensation mechanism means that a person could lose almost 50 percent of their lung function before feeling any symptoms.
There are many distinct types of lung disorders linked to different cell types, many of which have not been thoroughly studied. The complexity of the lung suggests that the ability to promote repair and regeneration versus contributing to disease-causing lesions may arise from very different cells. For this study, the team focused on mesenchymal cells, which are generally thought to play a supportive role in maintaining lung structure. They found five distinct cell types based on a suite of genes expressed by each. Of these five, they focused on two.
One cell type the Morrisey lab identified in the mouse lung that governs self-renewal of cell populations is called the Mesenchymal Alveolar Niche Cell (MANC). These cells are critical for the regeneration of lung alveoli. The second cell type is called the Axin2+ Myofibrogenic Progenitor cell (AMP), which generates cells called myofibroblasts that form scar tissue after injury, and likely contribute to diseases such as IPF.
The team analyzed what molecules these two cell types secreted and their surface cell receptors and compared this information to databases of known secreted molecules and receptors on adjacent cells. “One of the most important functions of these cells is to balance the repair and regeneration response after injury which occurs often due to the lung’s continual assault from the outside environment,” Morrisey said.
The “good” MANCs are found in niches or compartments near the alveoli to promote renewal of gas-exchange cells. They may play a key role in maintaining the alveoli during the normal life span of the adult. Dysfunction or loss of MANCs may contribute to diseases such as COPD, which involves loss of alveoli and decreased lung function. The role of the “bad” AMPs is to form scar tissue during wound healing. However, AMPs may grow out of control, potentially leading to diseases such as IPF.
Next, the researchers aim to identify these cell types in humans, working with associate professor of Surgery Edward Cantu, III, MD, the associate surgical director of Lung Transplantation. Morrisey says the Penn team wants to target MANCs for promoting regeneration while inhibiting AMPs to reduce the fibrotic response after injury. Knowing the detailed molecular differences between these two cell types should help in the next generation of targeted therapies such as nanomedicine.
These studies were supported by funding from the National Institutes of Health (R01-HL132999, R01-533 HL132349, R01-HL087825, U01-HL134745, U01-HL110942, T32-534 HL007843).
Coauthors, all from Penn, are Jarod A. Zepp, William J. Zacharias, David B. Frank, Christina A. Cavanaugh, Su Zhou, and Michael P. Morley.
Penn Medicine is one of the world’s leading academic medical centers, dedicated to the related missions of medical education, biomedical research, excellence in patient care, and community service. The organization consists of the University of Pennsylvania Health System and Penn’s Raymond and Ruth Perelman School of Medicine, founded in 1765 as the nation’s first medical school.
The Perelman School of Medicine is consistently among the nation's top recipients of funding from the National Institutes of Health, with $550 million awarded in the 2022 fiscal year. Home to a proud history of “firsts” in medicine, Penn Medicine teams have pioneered discoveries and innovations that have shaped modern medicine, including recent breakthroughs such as CAR T cell therapy for cancer and the mRNA technology used in COVID-19 vaccines.
The University of Pennsylvania Health System’s patient care facilities stretch from the Susquehanna River in Pennsylvania to the New Jersey shore. These include the Hospital of the University of Pennsylvania, Penn Presbyterian Medical Center, Chester County Hospital, Lancaster General Health, Penn Medicine Princeton Health, and Pennsylvania Hospital—the nation’s first hospital, founded in 1751. Additional facilities and enterprises include Good Shepherd Penn Partners, Penn Medicine at Home, Lancaster Behavioral Health Hospital, and Princeton House Behavioral Health, among others.
Penn Medicine is an $11.1 billion enterprise powered by more than 49,000 talented faculty and staff.